April 6, 2017, 11:30am
 |
| A little light reading before brain surgery |
We have learned so much about pre-op, people.
First off, nobody cares if you puke before surgery. You can have all the gastroenteritis you like out of either end, just don’t develop any respiratory symptoms within 2 weeks of your surgery date. I know this because, for 3 of Christopher’s 5 procedures, he’s had gastroenteritis the week of surgery. The PACU nurse said hopefully today’s surgery will stop all that. So maybe there’s a connection between Chiari and gastroenteritis. Christopher is certainly the most sensitive member of the family in that area.
Second, screw bedtime. Calories are way more important. If your child can eat until midnight, make sure they eat as close to that as you can get. Waiting in PACU before surgery sucks as an adult, nobody needs a hangry child. To this end, we took Christopher to Cold Stone Creamery and had him pick out a sundae at 9:45pm. He only ate half, but that’s okay, because then we started Pirates of the Caribbean and I handed him 3 buttered mantau (Chinese steamed buns) at 11:40pm.
Third, wake up early enough to get in 8 ounces of clear, sugary liquids at the last minute. We were told he could have clear liquids up until 2 hours before we had to report to the hospital at 6:45am. So at 4:15am, I woke that child up so he could come downstairs and drink 8oz gingerale before the cut-off. See, Calories are important, see above. Also, sore throats after intubation are Christopher’s primary complaint the first several hours he’s awake. He cared far less about the sore legs from the angiogram catheter or the headache from the brain surgery than he did the wick sore throat. Adding insult to injury, it was hours before they let him start sipping fluids or popsicles to ease that sore throat after the AVM surgery. So. Hydration.
Fourth, don’t let your older child fool you into thinking they don’t need stuffed animals for surgery. Maybe they no longer take them on vacation with them, but if fluffies still live on their bed, a few should go to the hospital. Heather Pitsenbarger and Summer Yen saved us last time by getting Christopher a giant orca (apparently the best body pillow ever) and a neuron (instant rapport with medical types). He initially told me he didn’t need them this trip, but when I countered, he didn’t insist. Both fluffies had prime positions in both his waiting room chair and on his PACU bed. The neuron, by the way, excited his anesthesiologist so much that she asked to photograph it. She’s also a brain researcher studying the effects of brain injury, so she’s now buying giant stuffed neurons for her researchh team this Christmas. (Side note: Are all Johns Hopkins anesthesiologists brain researchers? Or just the ones that work on neuro cases?)
 |
| Notice the critical placement of fluffies while he reads. |
Following these rules, for the first time ever, Christopher didn’t complain once about being hungry. They’re using a nasogastric tube instead of just an esophageal tube this time, so who knows what his throat will feel like. We may be trading a sore throat for a swollen nostril and a nose bleed. Just like last time, he’ll be under anesthesia long enough to wake up swollen and rashy, but it should dissipate within a few hours. The NG intubation is due to the fact that he’ll spend this surgery prone (on his stomach) with his head/neck pinned in place. The neck angle Dr. Groves wants isn’t conducive to a standard esophageal intubation. Having read his reports from the last two procedures before they came to visit us, the anesthesiology team was already prepared for Christopher to have emergence delirium and will give him fentanyl as necessary to prevent it. His bed in PICU has been confirmed and a very nice concierge spoke with us to see if we needed a tour. It wasn’t so scary watching Christopher shake as the nitrous oxide (laughing gas) took effect. For him, it’s a misnomer, it doesn’t make him slap-happy. As an observer, it would be easier to watch if he went to sleep via IV push. But he prefers they put the IV in while he’s asleep, and he’s a young enough patient, Johns Hopkins Hospital policy is to let him choose. As a parent, I try to give him agency over his body wherever possible, and this helps him feel like he’s got some measure of control over the situation.
Unfortunately, Christopher wasn’t quite able to finish The Fellowship of the Ring before his brain went mushy this morning (yeah, yeah, 4 hours’ sleep, blah, blah, blah). But he’s really close. He did, however, really make the anesthesiologists laugh when we were talking about their dosimeters and Marie Curie characterizing radiation. When noted that she got a unit of radiation named in her honor, he shot back with a crack about her dying of radiation cancer and a unit not doing her much good after she’s dead. Touché.
We are currently about an hour in to surgery. Dr. Groves did warn us that we may see a recurrence of some of the issues that cropped up after the last surgery because those neurons are weaker and more susceptible to injury. It would be a regression from his current baseline, not a complete re-injury, and since she made us wait so long between surgeries, it should be minor. But we did make sure he understood he could wake up with some left side weakness. The surgery won’t technically affect his vision or attention span, but until he clears the general anesthesia completely from his system, he might not be reading much. So we’ll take things as they come. He probably won’t be eating until tomorrow to prevent vomiting tonight as his body recovers from the initial shock of the decompression. Now we wait.
April 6, 2016, 2:30pm
Christopher is out!
 |
| Christopher is resting comfortably. Last time, he thought he'd sleep through PICU and not remember the experience. This time, when he had no expectation of it, he might well sleep through most of his time here! |
Dr. Groves removed the bone from his posterior fossa and C1 as planned. The dura was thickened and when she used the ultrasound probe after removing the bone, she found the CSF flow was still very restricted. So she placed a bovine pericardium patch during the duraplasty, which restored pulsation nicely. In the short term, this means Christopher will have more pain in recovery. There is now a risk for a CSF leak and meningitis (either bacterial or chemical) that wouldn't have existed without the duraplasty. The PICU attending is a seasoned physician who has treated lots of Chiari decompressions with duraplasty, however, so I feel confident we have an incredible team. They aren't too concerned about his blood pressure this time around, but are keeping the arterial line in to monitor his sodium levels, which can be problematic following duraplasty. The key to his recovery will be getting him up and walking tomorrow. Dr. Titsworth, one of the other neurosurgeons on the team, has already been in monitoring him for neuro and pain responses; we remember each other from the AVM resection.
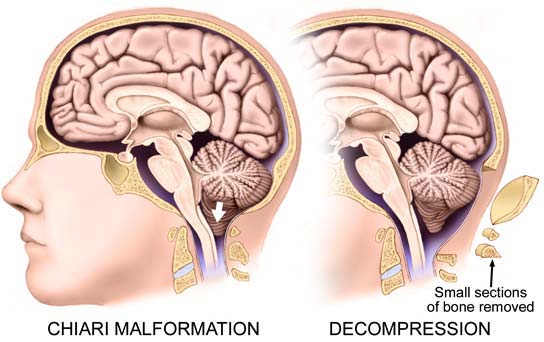 |
| This diagram shows the side view of where the posterior fossa was removed (craniectomy) and the spine of C1 (laminectomy). Image courtesy of Mayo Clinic. |
 |
| In this diagram, you can see where bovine pericardium (dura patch) has been stitched into the existing dura. Dr. Groves says she prefers bovine tissue because, in the ten years they've been using it, they see patient cells migrating into the patch and becoming one with the piece. It also, in her experience, produces the least amount of scarring. |
So far, Christopher is resting very comfortably and is just barely waking up. He reports a sore neck, but was able to prop himself up to swallow his acetaminophen dose at 2:00pm. The incision at the base of his neck is very minimal, they did a great job minimizing the stitches. The PICU attendings and resident spent a LOT of time asking "how we got to here", although it's obvious they read his whole file first. I think we got the A team, even his nurse seems more experienced than last time. He is on Dekadron (steroid) again for a few days to control inflammation, but no Keppra. He was given a large fentanyl bolus as he was exiting surgery to begin pain control as he clears the anesthesia. No emergence delirium today! I'd like to think he's just become a pro at this.
 |
| I'll try to get a better picture when he's awake and can turn over, but the incision site is much smaller than we anticipated. |
The pain management team has also been in to check on Christopher. In addition to IV valium around the clock to help with the neck muscle pain, they've given him a dilaudid PCA pump so that he can administer his own pain control. His respiratory rates are still pretty low (his computer isn't happy), but nobody seems too worried about it. They have his monitors silenced, so we hear the noises of the patients and practitioners on the floor, but no awful beeping.
It will be 2-3 months before we know what his new baseline is for headaches, but I'm hopeful we're almost off the Transsiberian Railway for good.
It will be 2-3 months before we know what his new baseline is for headaches, but I'm hopeful we're almost off the Transsiberian Railway for good.
Woohoo! That's awesome news!! Continued prayers. Hang tough 😘
ReplyDeleteWonderful! We'll keep praying for him! - Ender
ReplyDeleteGo Christopher! So glad to hear it went well <3 :)
ReplyDelete