Six and seven weeks’ Post-Op, October 10, 2016
Drs. Ahn and Tamargo couldn’t stop grinning, they were so pleased with his progress. They were so interested to know when he first walked without a wheelchair, and other questions. Dr. Tamargo did confirm all Christopher’s worst thoughts about neuropsychology by telling him their diagnoses are pure conjecture. Dr. Ahn was more careful, saying the testing was done too soon to be certain, and would need to be re-tested. They gave him full clearance to return to any and all of his previous activities, “as though he’d never had brain surgery”. A standard neurological exam (think touching your finger to your nose, walking a straight line) showed only minimal impairment.
Additionally, they took Christopher off Keppra. Hallelujah. Most of his taste issues went away within days, but his pediatrician, Dr. Kapoor, had to put him on Zantac to alleviate the severe stomach and intestinal pain. We nearly did testing for C. diff, but the Zantac kicked in so quickly it wasn’t necessary. I’ve fought reflux for decades, but I didn’t connect his pain to that, so I’m very grateful the pedi did. The anger and anxiety disappeared pretty quickly, too.
We saw Christopher's headache specialist October 10 and his physical medicine physician 1.5 weeks ago. Langdon says, night and day, he's a different kid than she saw this summer. Korth had only ever seen him the day after surgery when she assessed him and recommended he go to Kennedy Krieger for inpatient rehab. It took her 20 minutes to connect Christopher with the kid who couldn't move in the bed (he had a hoodie on, so no visible craniotomy scar). And then her jaw dropped.
While the neurosurgeons feel he can return to any activity he previously enjoyed as though he hadn’t ever had brain surgery, both Dr. Korth and Dr. Langdon have some concerns for getting him to the one-year surgery anniversary. But, as bad as things were, everyone is completely amazed at his recovery thus far. We are no longer walking through a living nightmare. Christopher's headaches and mental state are better than they've been in over a year. He still gets exhausted easily and we have to carefully plan his school day around outings and therapies.
There was some need for oculovestibular therapy to correct some residual vision issues from surgery. Luckily, his outpatient PT caught it and prescribed exercises so that they corrected before we were able to find and schedule OVT. Dr. Korth is also very concerned that his left ankle remains very weak, affecting his entire trunk balance and stability. She doesn’t want him participating in recess games like tag or soccer for a year. That did.not.go.well. She did give Christopher permission to begin a ballet class, so I’ve spoken with Skye Ballet, the studio Alexander attends, and they’ve agreed to let Christopher join.
N.B. His first class was a major success! He felt so good to be jumping without a spotter and to just be part of a regular, active, group of boys again. Furthermore, his behavioral psychologist is thrilled because of all the research showing major connections between ballet and memory. Win-win.
Three Months’ Post-Op, November 22, 2016
We had the first follow-up MRI today, along with appointments with Dr. Ahn, the vascular neurosurgeon, and Dr. Groves, the spinal neurosurgeon. When Christopher was shown the before and after images of his AVM site, he exclaimed, “Look! Even my ganglia have an Olympic sized swimming pool!” Such a swimmer.
More importantly, the MRI does.not.show any regrowth of the AVM. They can begin to regrow in as few as 30 days, so this was welcome news. The overall chance of regrowth is only 5-10%, so Dr. Ahn is optimistic it will never be an issue again. Still, Christopher will need a repeat cerebral angiogram when he’s 15 to make sure. That way, if it does return, there’s time to remove it and rehabilitate without affecting Christopher’s trajectory for college. Again, Dr. Ahn smiled during the entire exam. He’s a fairly quiet Asian man, so it’s amazing to watch how pleased he is with Christopher’s progress. Honestly, we are, too. The brain of a little kid is a truly amazing thing….
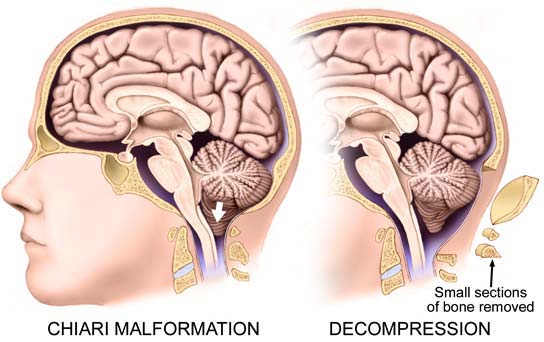
Dr. Groves’ appointment wasn’t until after lunch, after we’d done the first two appointments. Christopher grew noticeably quieter and more agitated as it approached. We were really hoping she’d be ready to schedule a Chiari decompression in January, Christopher has been working really hard in PT and in shortened swim team practices towards that goal. Dr. Ahn had just told us he saw no reason to wait any longer, he’s fully healed from the AVM procedure. But no. Dr. Groves, we’ve learned is extremely methodical. But we met a patient at Kennedy Krieger who, despite a devastating spinal cord injury from a motorcycle accident, will walk again because of her caution and skill. So, while Christopher really hates her pace, he has the utmost trust in her abilities, thanks to a 21 year old’s recovery. Hindsight being 20/20, we also feel that she was probably more honest with us regarding just how tough the AVM surgery was going to be than the vascular docs.
At this appointment, she warned us that she thinks she can make the headache spikes go away with surgery, but not necessarily move the baseline lower than what he achieves with acupuncture. His rehab physician said the same thing in December. Furthermore, because general anesthesia itself causes memory, attention, and appetite changes, Dr. Groves wanted Christopher to wait 6 months from the AVM resection to be put under again. There is evidence in children that too many anesthesia events, too close together, can make the changes permanent. He'd just started doing regular swim practices again, but only at 30 minutes, so she also wanted him swimming full practices before another surgery as an indicator he was back to his pre-surgery strength and conditioning. She doesn't anticipate he'll need PT this time, although she always requests a PT consult in hospital, but she does want him to be as strong as possible before he goes through another major surgery that will sideline him for 6-12 weeks. She did discuss details of the surgery with us, so I don't think she doesn't want to do it at all, just that she is very conservative and doesn't want to create unreal expectations.
Six months' Post-op, February 3, 2017
Christopher's recovery remains pretty spectacular. To look at him, only his PT knows his weaknesses, and maybe his swim/ballet teachers. We even took him skiing in January! His first ski day, at Bryce Resort, was a bit bumpy, because he lacked the muscle memory for turns using the left leg. A semi-private lesson with his brother cured than in under 90 minutes and he was back to skiing greens like a pro. Two weeks' later, we went to Snowshoe for the week, and when he was bored of greens, a semi-private lesson to clear him on blues was in order. He had trouble in the lesson putting together the components of parallel turns, instead of the snowplow turns he's used up to this point. But the next day, he nailed it and was flying down the mountain with great control--and parallel turns! He also went swimming, climbed the rock wall, spun in a Eurobungy that week. We didn't plan the trip to coincide with the six month anniversary of the AVM surgery, but it was a great way to spend the week. Rehab medicine and PT have, obviously, now cleared him for all but heavy contact sports.
Christopher's headaches are fairly stable. His baseline Chiari pain has bumped up a bit to a 2/3 now that he's doing full swim team practices, skiing, etc. He has a Chiari headache spike to a 7/8 on co-op days and whenever the barometer is very high or low (strong storm system days), so at least 2 days a week. He isn't having full-blown migraines, but does get small break-through ones on bad barometer days. The craniotomy site also often develops a headache on storm system days, but his neurologist feels his head is young and plastic enough, it will fade with time and not be a permanent weather vane. He is still doing acupuncture every 2 weeks.
Christopher has a full school schedule and is doing great in his school work. Many days we have to play Tetris with the order of his work to compensate for his energy level. Mondays always cause trouble because he swims for an hour, then goes straight to PT, and comes home physically exhausted. So he does a lot of reading and some of the written work has shifted to other days. When I told his neurologist my concerns that, at current stamina levels, he'll have trouble completing high school and college coursework, Dr. Langdon assured me it isn't problematic. She has high hopes for Chiari surgery (more on that later), but says that she has lots of chronic headache patients without a surgical option, and she writes 504 accommodation plans for them even in college. Mostly, she eliminates busy work and asks, for example, for 20-30 core quality math problems instead of 50 total. This is pretty much what I've done with his schedule, so that's comforting. English is a bare-bones reading and handwriting operation at this point, with his Latin studies doing all the heavy-lifting for grammar and vocabulary. Comprehension and composition come primarily mostly through his history activities.
We discussed all this with Dr. Langdon this week. She agrees with everything Groves told us, but doesn't think there's a reason for further delay or to avoid surgery altogether, now we're beyond the 6 months. She thinks he will get significant relief from surgery, even of the baseline, but thinks he'll likely always be a headache patient. Migraines, once triggered, often don't just disappear--even if you remove the proximate cause. Langdon thinks revisiting Moores, the Inova neurosurgeon, could help us feel more comfortable with specifics, but would prefer Johns Hopkins do the procedure since that clinical team has all the notes and experience of his last surgery. Since she has privileges with Children's National and Inova, not Hopkins, this advice is not earning her money.
The symptoms that earned Christopher an EEG are periods of 5-7 days of extreme clumsiness that happened in October and then in November. I initially thought they were occurring because he was spending less time resting on the couch between school and PT activities, his brain was having to work at a new speed to control his body, and needed to learn to work faster. This is the AVM recovery/multi-tasking explanation. Growth spurts also cause clumsiness, and he's grown nearly 3 inches the last six months. Langdon says they could have coincided with really bad headache weeks, as well. Chiari malformations can put enough pressure on the brain stem to cause clumsiness, too. But around Christmas, he started dropping things with just the right hand. It went from every few days, to daily, to twice daily over three weeks before I called his pediatrician. She was very concerned because it wasn't bilateral and asked me to call Langdon because she thought he needed new brain scans. Langdon agreed and sent us to the ER for an MRI with contrast. That was clear of any signs of swelling or bleeds. The Chiari looks the same as last April. In the absence of a structural cause for the clumsiness, Christopher is probably normal for him. But since major brain surgery can cause seizures, and small seizures can present as clumsiness, Langdon felt an EEG was in order. We'll get those results in 10 days. When I called Johns Hopkins to schedule his next appointment with Groves after the MRI, I told the secretary briefly about it, she spoke with Stephanie, our favorite PA, and they asked he be seen this month instead of in the next three. That is scheduled for Feb 28.
N.B. Those EEG results were also normal.